


Myelomeningocele
Myelomeningocele is a type of spina bifida. This is when the neural tube has failed to close and the neural tissue is exposed on the baby’s back. The myelomeningocele will look like a sac sticking out from a baby’s back.
In early development, the brain and spinal cord start as a tube-like structure called the ‘neural tube’ that is open at either end. These openings close within the first weeks of pregnancy, and the neural tube continues to grow and fold, eventually forming the brain and spinal cord.
If the tube fails to close properly, this results in a group of problems called ‘neural tube defects’. There are two types of neural tube defect: open, also called spina bifida aperta or myelomeningocele, or closed, also called spina bifida occulta.
This information explains about the open myelomeningocele type, which accounts for 75 per cent of all cases of spina bifida.
In myelomeningocele, the neural tube has failed to close and the neural tissue is exposed at a place on the baby’s back called the ‘neural placode’. This most commonly happens in the baby’s lower back just above the bottom, but could occur anywhere along the spine. The myelomeningocele will look like a sac sticking out from the baby’s back.
How is myelomeningocele treated?
Without the protective covering of skin, the spinal cord will become further damaged, spinal fluid often leaks from the area and there is a very high risk of infection. Surgery is usually recommended within the first few days of life.
The aim of surgery at this stage is to put the spinal cord back into the spinal canal and repair the defect in the back so that the area is covered with normal, healthy skin.
Before surgery, the affected area is covered with a dressing and the baby will be nursed on their front. A number of specialists will visit to examine the baby, including a neurosurgeon, physiotherapist, paediatrician, orthopaedic surgeon and anaesthetist.
Tethered Spinal Cord
What is a tethered spinal cord?
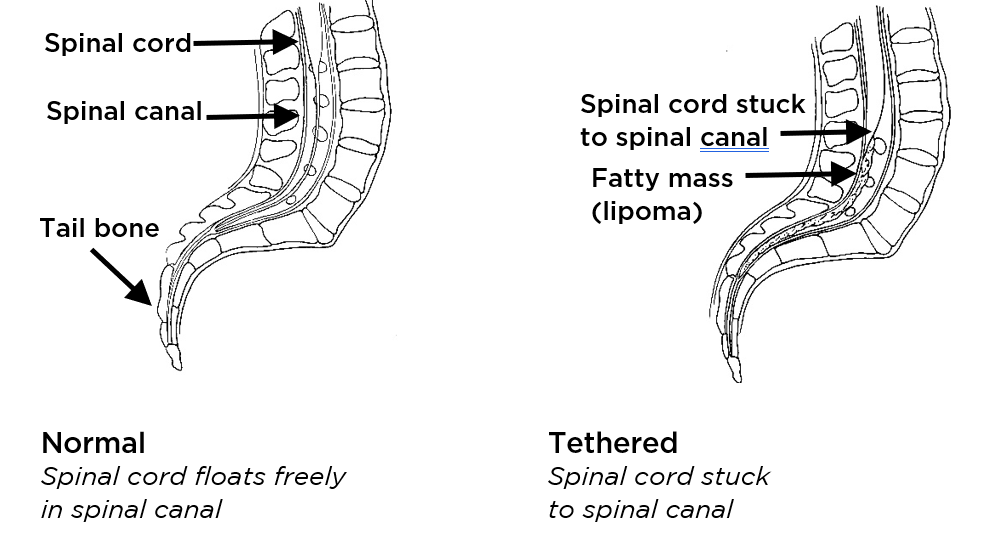
Normally, the spinal cord floats freely inside a tube in the spine called the spinal canal. A tethered spinal cord is pulled down and stuck to the inside of the spinal canal.
As a child grows, a tethered spinal cord will stretch like a rubber band. If the problem is not treated, it can cause lasting damage to a child’s spinal nerves. This can lead to loss of function, like the ability to walk or control their bladder.
Tethered spinal cord most often happens in children who are born with problems affecting the spinal cord, such as:
- A small sac sticks through an opening in the spine (myelomeningocele). This is the most serious form of spina bifida.
- A fatty mass is attached to the spinal cord (lipomyelomeningocele).
- The very end of their spinal cord is held down too tightly because the flexible fiber connecting it to the bottom bones of the spine is thicker than normal (fatty filum).
In a child born with such a condition, their spinal cord may become stuck, or tethered, to the fatty filum, myelomeningocele or lipomyelomeningocele. This pulls on the spinal cord as the child grows, causing symptoms.
A child also may have a tethered spinal cord because:
- They have a small abnormal channel from their skin into their spinal canal (dermal sinus tract)
- Their spinal cord is split into 2 cords near the end (diastematomyelia)
How is tethered spinal cord diagnosed?
We bring together experts in Neuro Associates diagnose your child.
Our doctors:
Examine your child, looking for signs and symptoms
Use MRI (magnetic resonance imaging) to take high-quality pictures inside your child’s body to help us assess your child’s condition